
Medi-Cal’s introduction of new benefits and services – Enhanced Care Management (ECM), Community Health Workers (CHWs), and Community Supports – represents an enormous opportunity for children, youth, and families involved in child welfare. By addressing social determinants of health like food, housing, and safety and making connections to services that mitigate the impacts of trauma, ECM, CHW, and Community Supports are important new tools to propel system-involved children and families toward stability and healing.
Yet, despite being a targeted population of focus and categorically eligible for ECM, a small fraction of children involved in child welfare are receiving ECM services.
Major system changes take time to understand and adopt, but children and families involved with child welfare urgently need additional supports and resources. Increasing linkages to these new services for impacted children and families requires new collaboration between county agencies, managed care plans, and providers.
Full Circle wrote a white paper to summarize the barriers we see to increasing enrollment and to make specific recommendations for actions that would leadto more children and families accessing these important services.
Download the white paper here.
These insights are based on our experience at Full Circle Health Network collaborating alongside our 100-plus provider partners, multiple Medi-Cal managed care plans, and dozens of counties to serve thousands of children and youth over the last year and a half.
Full Circle was created by and for community-based organizations (CBOs) that have decades of experience providing trauma-informed care to children, youth, and families via contracts with county child welfare and behavioral health departments. These provider agencies pioneered complex care models for youth, and their collective experience connecting, collaborating, and coordinating among child-serving systems is the foundation for successful ECM delivery.
The Nation’s Largest Child Welfare System: Understanding the Population
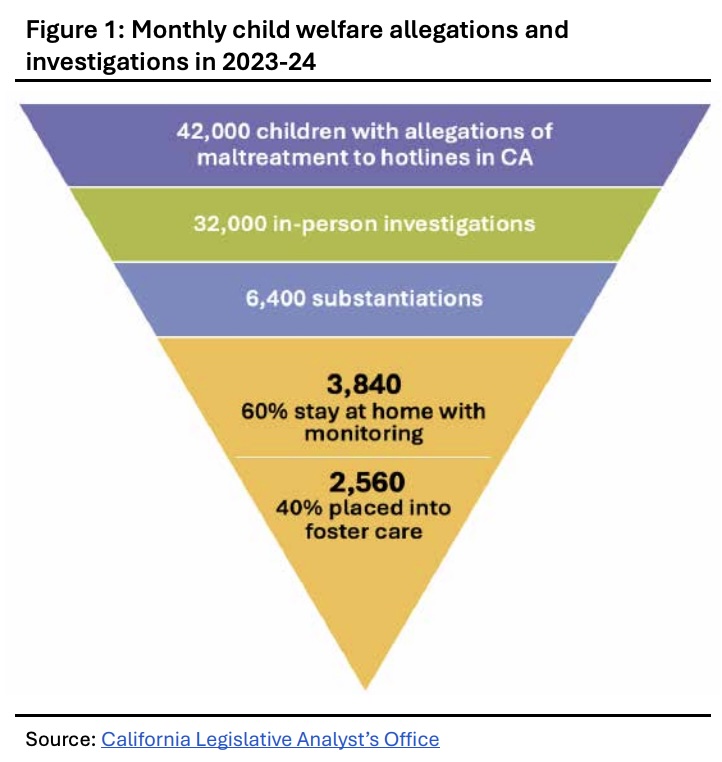
Each month nearly 100,000 children and their families interact with California’s 58 county child welfare agencies, according to the California Legislative Analyst’s Office. The impacted families are disproportionately people of color and low-income.
California’s number of children in foster care decreased by 28% over the last decade to 40,165 children in October 2024 – an all-time low. This shift to preventing system involvement and reducing family separation is a national trend. In California, counties have developed comprehensive prevention plans and are implementing community pathways to services that promote prevention and family stability.
About 80% of child welfare cases originate from allegations of neglect – not abuse. Interpersonal violence, mental health disorders, and substance use disorders frequently are co-occurring risk factors. Substantial evidence exists that child abuse and neglect can be prevented by helping caregivers meet their families’ concrete needs, such as housing, food, transportation, and child care, and help them access services to address their complex risk factors. These concrete needs are also social determinants of health.
Medi-Cal plays an enormous role in promoting family stability. About half of California’s youth in foster care come from families with incomes less than $12,000 annually, and most others have household incomes low enough to qualify for Medicaid. Thus, nearly all children, and often their parents and caregivers, qualify for Medi-Cal prior to any child welfare system involvement.
About one in three children in foster care are younger than age five, underscoring that support for these children requires supporting parents and natural support systems.
At the Intersection: Child Welfare and Enhanced Care Management
As with most social safety-net programs in California, responsibility for child welfare services delivery has been “realigned” to county child welfare agencies. All children in foster care are eligible for Medi-Cal, and eligibility is determined at the county level.
Medi-Cal’s new enhanced care management benefit was created to help individuals with complex needs navigate systems, programs, and providers. Children and youth in foster care, formerly in foster care or in family maintenance are automatically eligible for ECM. ECM case managers aim to help program enrollees identify and close service gaps and improve coordination across a child’s and/or family’s medical, behavioral health, and social services delivery systems. ECM services should augment any existing case management efforts and promote effective, timely communication.
ECM has great potential to bolster capacity of child welfare case workers and public health nurses improving their job satisfaction and promoting their ability to support children and families along the entire service continuum.
Critically, ECM is a sustainable funding source for community-based organizations doing family systems work. We are hopeful that child welfare agencies increasingly view ECM as an additional support tool.
Targeted ECM Goals for Child Welfare
No targeted goals for ECM utilization rates among the child welfare population exist. We believe setting considered targets for subgroups within the child welfare population is useful. If targeted utilization rates were achieved, about 45,000 child welfare involved children and youth would be enrolled in ECM, requiring about 1,125 lead care managers (at a ratio of 1:40), a 26-fold increase over numbers reported in June 2024.
Systemic Drivers Behind Low ECM Enrollment
Full Circle has observed several factors contributing to slow uptake among child welfare impacted youth and families. We summarize and offer recommendations to address them within the full document.

Conclusion
Any major system change takes time to understand and adopt, but children and families involved with child welfare are at a significant crisis point in their lives and urgently need additional support and resources. Medi-Cal’s introduction of ECM, CHWs, and Community Supports represents an enormous opportunity. Successful adoption requires new collaboration between county agencies, managed care plans, and providers. Implementing recommended actions will result in linking more children and families to necessary services and increase their trajectory toward maintaining safe, stable, and nurturing relationships foundational to mitigating trauma and promoting long-term wellbeing.
Acknowledgements
We express gratitude to the UCAAN ACE’s Aware Funding Initiative, PATH CITED program at DHCS, Medi-Cal health plans, network providers, and the California Alliance of Child and Family Services for their contributions and support.