California's Enhanced Care Management (ECM) program was built for adults. The metrics reflect that. The frameworks reflect that. Even the assumptions baked into ECM, from reducing inpatient hospitalization, managing chronic disease, promoting medication adherence, are adult-oriented by design.
Yet lost in this is the fact that thousands of California's most vulnerable children and youth are now being served through ECM. There is not a shared definition of what "success" means for them. Treating children like small adults is not the answer.
Filling a Gap
ECM grew out of California's Whole Person Care pilots and health home programs. These models were real innovations, but when ECM was extended to children and families, the underlying theory of change never caught up.
Full Circle spent the past year building a theory of change while helping dozens of community-based providers deliver ECM to thousands of children, youth and families.. Our new white paper, Enhanced Care Management: A Theory of Change for Children, Youth, and Families, lays out a logic model framework grounded in child development principles, trauma-informed practice, and the lived realities of the communities we serve.
Why a Theory of Change Matters
A Theory of Change isn't an abstract exercise. It's a working document — a communication tool, a planning framework, and an accountability structure all at once.
For ECM, a theory of change is a comms tool, a planning framework, and an accountability structure all rolled into one. It does something urgently needed: it answers the question “what are we actually trying to achieve?” before deciding how to measure it.
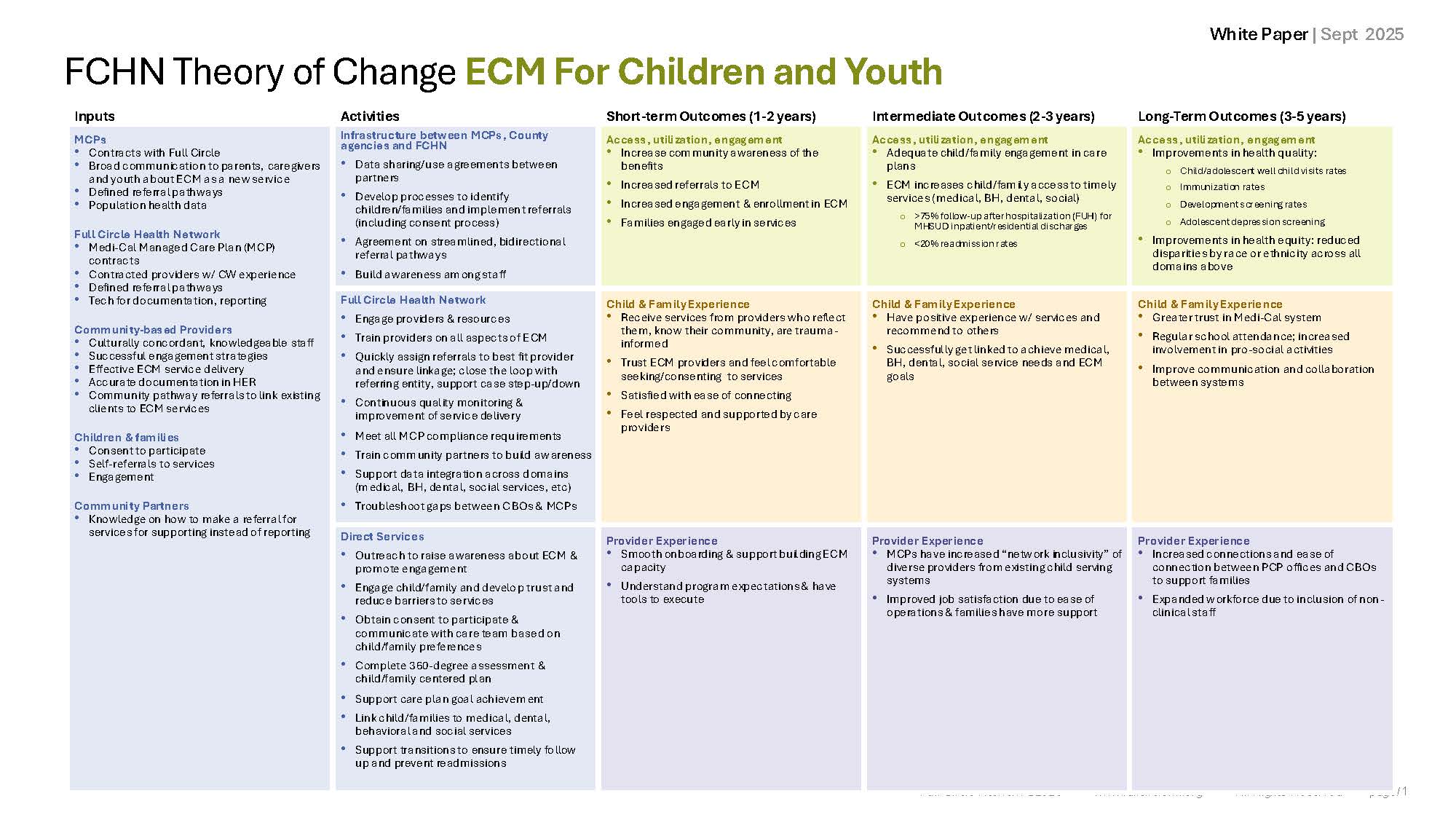
Our framework organizes outcomes across three lenses:
- Access, utilization, and engagement Are families finding ECM? Are they staying connected? Are referral pathways working?
- Child and family experience Do families feel respected, heard, and supported? Do they trust their providers? Would they recommend the service to others?
- Provider experience Are community-based organizations successfully onboarded? Are they gaining capacity, not just compliance requirements?
These three lenses operate across a timeline: short-term (1-2 years), intermediate (2-3 years), and long-term (3-5 years) outcomes. The logic model diagrams, available with this white paper, show how inputs and activities connect to outcomes across both the general ECM population and specifically for child welfare- and justice-involved youth.
Built on Evidence but Centered on Children
Full Circle's Theory of Change is not invented from scratch. It draws on a substantial research base:
- The American Academy of Pediatrics calls care coordination bridging medical and social systems an essential component of serving children with high needs.
- Research on parent empowerment shows that addressing barriers, including stigma and distrust of providers, leads to better service utilization across generations.
- California's own ACES screening experience shows that without robust referral infrastructure, evidence-based screening doesn't translate to family support.
ECM, when delivered correctly, is that infrastructure. It creates the connective tissue between pediatric providers and the community-based organizations best positioned to meet families where they are.
Five core principles anchor our framework:
- Family-Centered Approach: Recognizing that children's health
and well-being are inextricably linked to family functioning and stability. - Trauma-Informed Care: Understanding that many families accessing ECM have experienced inter-generational trauma that affects their engagement with systems.
- Prevention Focus: Emphasizing early intervention to prevent escalation
of health, behavioral, and social challenges. - Cultural Responsiveness: Ensuring services reflect the language and cultural backgrounds and preferences of the families served.
- Systems Integration: Coordinating across child welfare, healthcare, education, and community support systems.
Two Populations, Two Logic Models
This post includes two detailed logic model diagrams:
- ECM for Children and Youth (General Population) traces how coordinated outreach, community-based providers, and managed care partnerships can drive improvements in well-child visits, immunization rates, developmental screenings, and adolescent depression screening, alongside reductions in hospital readmissions and emergency department overuse.
- ECM for Child Welfare and Justice-Involved Youth goes further. This population faces compounded barriers: system involvement, placement instability, interrupted care, and, for older youth, the looming transition to adulthood without a safety net. The logic model for this group emphasizes preventing re-entry into the child welfare system, supporting family reunification, and empowering Transition Age Youth (TAY) and Non-Minor Dependents (NMD) to navigate their health plans with confidence.
You can find our White Paper and Theory of Change tables on our resources page at fullcirclehn.org/resources